1.WHAT
ARE PRESSURE ULCERS ?
A
pressure ulcer is an area of localized damage
to the skin and underlying tissue caused by
pressure, shear, friction or a combination
of these (EPUAP 1998). They are most likely
to occur when a hard bony area covered by
a thin layer of tissue is in contact with
a hard surface, such as a bed, trolley, theatre
table, wheelchair etc.
The body can withstand high interface pressures
for a very short period of time. It is when
the pressure is not regularly, relieved that
damage occurs and a pressure ulcer develops.
Elderly patients are particularly vulnerable
because their skin usually becomes thinner
and more fragile with age. Pressure sores
can develop in a matter of hours. Decubitus
ulcers can happen during hospitalization,
in a nursing home or in a community setting.
|

4 Stages of pressure sore development
|
|
| |
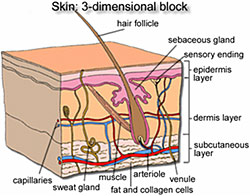
STRUCTURE OF THE SKIN |
The skin is essentially
our largest organ and made from three distinct
layers. The top surface called the
Epidermis which is rough and microscopically
thin, this is constantly being worn away and
replaced throughout our life span. Underlying
the epidermis is viable dermis consisting
of nerves, glands, fatty (adipose) tissue
and muscle. Beneath the dermis is a subcutaneous
layer of adipose tissue containing a large
number of blood vessels. |
| PRESSURE
SORE SYMPTOMS |
Common Areas For sore Development |
| Unrelieved pressure
on a specific area of the body (eg the heels
, the hips) will affect the blood supply to
the skin and underlying tissues causing that
area to become damaged. Mild tissue damage
results in skin discoloration, giving a brown
or purple appearance. This may look darker
if the skin is very fair.
More severe pressure ulcers can expose
muscle and even bone. The area around the
dead tissue will look red and inflamed and
may become infected. This process, once
occurred is extremely difficult to heal.
The resulting wound can be very painful
and can eventually lead to death. Most pressure
sores can be prevented. |
| |

Stage One Pressure injury Early Sign |
 |
|
| COMMON LOCATION
FOR PRESSURE SORES |
Sitting Position |
Prone Position
|
Lateral Position |
Lying Position |
| 2.PREVENTING
PRESSURE SORES(Skin Inspection & Repositioning) |
Skin Inspection
Patients skin and pressure points should be
inspected regularly. Each patient should have
their vulnerable areas checked i.e. heel,
sacrum, femoral trochanters any area which
is in contact with pressure or where shear
and friction are exerted. Patients should
be encouraged to inspect their own pressure
points where possible.
REPOSITIONING
In order to prevent pressure ulcers developing,
it is important that those who are immobile
have their position changed at least every
two hours.
This may need to be more frequent if sitting.
Those at higher risk of pressure ulcers,
such as the elderly and those with existing
medical conditions should keep as active
and mobile as possible.
Also important is keeping the skin clean
and dry, and checking that bed linen is
free from wrinkles.
EQUIPMENT PROVISION
Pressure reducing/relieving devices
There are many different types of support
surfaces which can either reduce or relieve
pressure.
Pressure Relieving mattresses come in many
different forms and these are seen to reduce
pressure.
PRESSURE RELIEVING MATTRESS
Pressure relieving mattresses are made
of rows of air cells, these cells inflate
and deflate (alternate) sequentially in
a set time period, this ensures that pressure
on the body will be continually changing
and area’s of the body for a period of time
will have pressure relief.
Pressure relieving mattress are controlled
by a powered intelligent pump system, Most
system’s have features which enable the
user to alter the comfort setting for patient.
Alternating Pressure relieving mattress's
also can have small ventilated holes within
the cells to gently allow air to escape
to reduce any skin moisture and also to
increase the comfort for the patient
|
EARLY SIGNS OF PRESSURE SORE FORMATION
The skin around the area will be red and shiny
or dark purple.
The skin may be warm to the touch compared
with nearby tissue.
The area may also be swollen or hard and may
lack feeling.
Note: Skin reddening that disappears after
pressure is removed is normal and is not a
pressure ulcer. Discoloration of the skin
that is constant may be a pressure ulcer.
|
|
Grade 1:
The skin is not broken but the color of the
skin changes, purple or red. The irritated
skin may feel warmer than the skin around
it. At this stage, the pressure ulcer may
be healed just by taking pressure off that
skin area. Non-blanching hyperaemia / erythematic
of intact skin demonstrates that damage is
occurring (EPUAP 2001) |
|
Grade 2:
Partial thickness skin loss involving epidermis,
dermis or both superficial damage presenting
as blister or abrasion (EPUAP 2001) |
 |
 |
| The
skin may break or blister and the skin
around it will look irritated and inflamed.
|
|
Grade 3:
Full thickness skin loss involving damage
to, or necrosis of subcutaneous tissue that
may extend down to, but not through, underlying
fascia (EPUAP 2001) |
|
 |
| Damage
to the body tissue begins to develop
and the sore becomes more than a surface
wound as it affects the tissue underneath
the skin. At this stage the sore will
have a crater-like appearance. |
|
Grade 4:
Extensive destruction tissue necrosis or damage
to muscle, bone, or supporting structures
with or without full thickness skin loss (EPUAP
2001) |
|
 |
| The
ulcer has eroded deeply, causing damage
to body tissue, bone, muscle, tendons
and joints. The risk of infection is
much higher at this stage |
|
Extensive destruction tissue necrosis or damage
to muscle, bone, or supporting structures
with or without full thickness skin loss (EPUAP
2001)
Product Usage Key..
|
|
|
|
|
| Strongly Recommended |
Recommended |
|
Not Recommended |
|
| |
|
Prevent |
Grade1 |
Grade2 |
Grade3 |
Grade4 |
| #Economic |
 |
|
|
|
|
|
PL8530 |
 |
|
|
|
|
|
PL8535 |
 |
|
|
|
|
|
PL8900PLUS |
 |
|
|
|
|
|
Cushion |
 |
|
|
|
|
|
|
|
|
| |
|